We explain the different types of immunotherapy treatment for cancer patients, and what our researchers are currently working on in this area.
We explain the different types of immunotherapy treatment for cancer patients, and what our researchers are currently working on in this area.

Immunotherapies are treatments that use the immune system to target and destroy cancer cells. They are a rapidly growing and exciting area of breast cancer research. The following blog explains the different types of immunotherapy treatments.
The immune system – our guardian protector
Our immune system is made up of specialised cells, tissues and organs that work together to protect us from disease. The cells of our immune system are called white blood cells.
T cells are a type of white blood cell that recognise unfamiliar substances, germs and abnormal cells like cancer cells. They can trigger an immune response to fight infection and illness. If the body faces a threat it has seen before, the immune system can recognise it and respond immediately.
Usually, the immune system can also identify and destroy malfunctioning cells. However, occasionally it misses the mark, and this is when cancer can start developing. Immunotherapies aim to harness the power of the immune system by stimulating it to recognise and act against cancer.
Immune checkpoint inhibitors
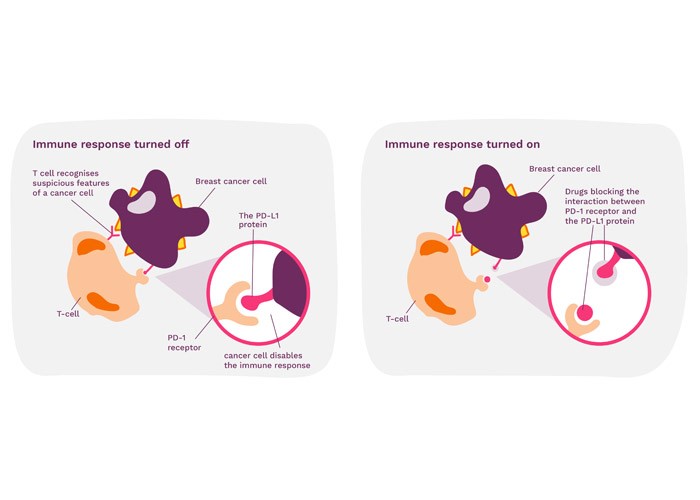
PD-L1 is a protein that stops the immune system from attacking healthy cells in the body. Found on the surface of cancer cells, PD-L1 interacts with receptors on the T cell to disable the body’s immune system.
Immune checkpoint inhibitors are a group of drugs that work by blocking the interaction between cancer cells and T cells. When this interaction is blocked, the cancer cells can no longer switch off the T cells and the immune system is activated, allowing it to find and destroy the cancer cells. However, some cancer cells do not make PD-L1 and this means that immune checkpoint inhibitors cannot be used for everyone.
The immunotherapy drug atezolizumab (Tecentriq) is currently used to treat some breast cancers. Pembrolizumab is a similar drug that is in clinical trials for treatment of triple negative breast cancer. Early results suggest that it could be used before surgery to treat primary breast cancer and people with secondary breast cancer.
Monoclonal antibodies
Antibodies are molecules made by the immune system. Monoclonal means that they recognise the same feature of the same molecule. Monoclonal antibodies can be made in the lab to specifically recognise molecules found on the surface of cancer cells.
Monoclonal antibodies are already used to treat breast cancer in several different ways. The drug trastuzumab (Herceptin) is a monoclonal antibody used to treat HER2 positive breast cancer. Trastuzumab works by attaching itself to the HER2 molecule found on the surface of breast cancer cells. This stops breast cancer cells from growing. It also helps the immune system to recognise and destroy breast cancer cells.
Monoclonal antibodies can be joined to other cancer drugs so that the drug is delivered directly to cancer cells. This makes the treatment more targeted, reducing the side effects. For example, trastuzumab emtansine (Kadcyla) is a combination of trastuzumab (a monoclonal antibody) and a drug called emtansine (DM1). DM1 works by stopping the cancer cells from dividing.
More monoclonal antibody treatments are currently being developed and tested to treat breast cancer. A drug called trastuzumab deruxtecan, or T-DXd, has shown promise in clinical trials to treat people who have already received several treatments for secondary HER2 positive breast cancer.
Professor Sophia Karagiannis, a Breast Cancer Now researcher, is working to develop monoclonal antibodies that can recognise triple negative breast cancer.
CAR-T cell therapy
CAR-T cell therapy is a treatment that involves taking a sample of T cells from a person. These T cells are then modified in a lab to make a protein called CAR. This protein makes the T cells better at recognising cancer cells. Large numbers of these T cells are then grown in a lab before they are given back to the person.
This treatment is not currently available for breast cancer, but early research shows that it may be effective for treating triple negative breast cancer. Dr John Maher, a Breast Cancer Now researcher, is developing a CAR-T cell therapy for HER2 positive breast cancer.
Another approach to T cell therapy has recently shown potential in breast cancer. Rather than altering patient’s T cells, researchers used highly sophisticated methods to select the T cells which naturally have the highest ‘anti-cancer’ potential. They were grown in the lab to increase their numbers and then used as a treatment along with a checkpoint inhibitor drug. Only one patient with secondary breast cancer was treated this way.
Another Breast Cancer Now researcher, Professor Andrew Sewell from Cardiff University, is trying to understand how a special group of T cells can recognise the difference between cancer cells and healthy cells.
Cancer treatment vaccines
Vaccines prevent infectious diseases by giving someone a part of a virus or bacteria that does not cause harm so that the immune system can learn to recognise and fight it. Cancer treatment vaccines work in a similar way but are designed to treat the disease rather than prevent it. They aim to reactivate the immune system against cancer.
This treatment is not currently available to treat breast cancer. However, early clinical trials of treatment vaccines for cancer are currently underway. There are three types of cancer vaccines that look promising.
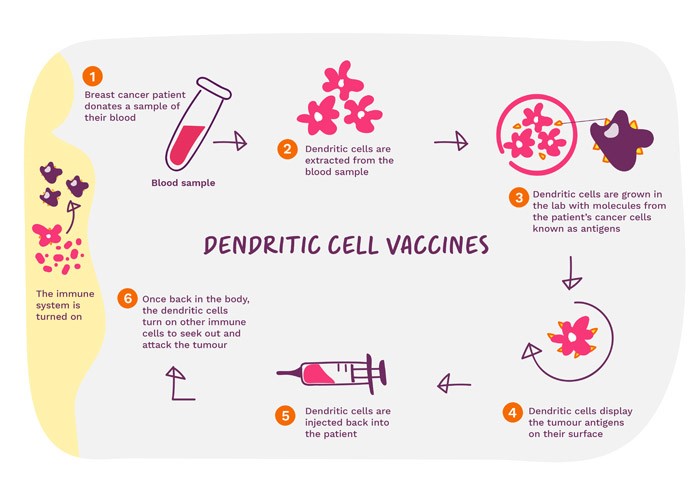
- Dendritic cell vaccines – dendritic cells (DCs) are messengers in the immune system and help T cells to recognise harmful cells. DCs are grown in a lab after being isolated from a person’s blood sample and they are exposed to molecules found on cancers. They are then given back to the person where they help T cells recognise cancer
- Antigen vaccines – train the immune system to recognise molecules that are only found on the surface of cancer cells. Large amounts of these molecules are made in the lab before they are given as a vaccine where they will hopefully help the immune system to recognise cancer cells. It’s early days but researchers are working hard to see if this vaccine could work for breast cancer.
- DNA vaccines – made up of fragments of DNA from the cancer cell, it helps the immune system to recognise proteins found on cancer cells by providing the instructions that make them. There has been limited success so far, but as we identify the genetic codes for more cancer proteins they could become more effective. There are also similar vaccines that use another type of genetic code called RNA.
The future of immunotherapy
There are advantages to immunotherapies:
- They tend to have fewer side effects than chemotherapy
- They can be given to people who have had chemotherapy or radiotherapy to prevent the cancer returning (recurrence)
- They have the potential to be longer lasting because immunotherapies train the body’s immune system to recognise and destroy cancer cells
However, people who have autoimmune disorders may not be able to take immunotherapies. Also, we do not currently know why immunotherapies work well for some people, but not others.
As more immunotherapy clinical trials are completed and scientists find ways to improve these treatments, we are hopeful that more immunotherapies will become regularly used to treat breast cancer and help save lives in the future.
Right now, we’re funding over 80 cutting-edge projects worth just over £29 million to discover how we can prevent breast cancer, save lives, and help people to live well with and beyond the disease.